Fluoride Alternatives

Fluoride Alternatives
As dental professionals, we have known that fluoride continues to be our number one defense in the prevention and progression of dental caries. The first fluoridated community water systems that began in 1945 in Grand Rapids, Michigan, continue to be recommended by practically all public health, medical, and dental organizations, including the American Dental Association, the Canadian Dental Association, the American Academy of Pediatrics, and the World Health Organization (WHO).
Fluoride, although most beneficial in community water systems, is an added ingredient in patient home care products and is included in dental preventive treatment procedures. Whatever distribution or application process method, fluoride continues to be a cost-saving, safe, and effective anti-caries intervention 1
Our patients, however, have become suspicious, have acquired certain beliefs, or have been influenced by fluoride opponents who wage controversial opinions and data on the safety of fluoride. It is not surprising when patients refuse fluoride treatments for themselves or their children.
The misrepresentation of fluoride exposure by the media and interest groups has made it a difficult conversation to have with some of our patients. But we must accept that patients have the right to refuse to use fluoridated products or have fluoride applied in a clinical setting. It may be possible in some cases to educate the patient with evidence-based data to convince them that fluoride has been proven to be a safe, practical addition to caries prevention.
If your patient expresses concerns or questions about fluoride, the best thing to do is to listen to their reasoning. Understanding why and how a patient has decided to avoid fluoride can provide a segue to a productive conversation rather than a debate. Asking them where they retrieved the information can help you respond appropriately. Fears of toxicity, necessity, the thought that fluoride is only for children, consequences, and insurance coverage are some reasons for fluoride refusal. Responding to these concerns with suitable answers may influence or change a patient's attitude toward fluoride.
Refusal of Fluoride
For those patients who adamantly refuse to use fluoride in any form, we must be knowledgeable in guiding them to alternative methods to increase their resistance to and prevention of caries.
Prevention of dental caries involves many aspects.
Primary prevention involves the etiology of the disease. The etiology of caries is based on a theory that requires the interaction of oral microorganisms, fermentable carbohydrates, oral environment, host, and time.
Primary prevention seeks to alter the microorganisms in plaque formation, reducing sugar exposure and strengthening the teeth.
Primary prevention that changes one or more of the factors in the decay equation can include education in fermentable carbohydrate consumption, frequent disruption of the plaque biofilm, and systemic disease management.
These modifiable components can improve and change the caries risk as long as the behaviors continue. Addressing primary caries risk factors can change the oral environment before damage from caries is evident. In addition to primary prevention, such as dental sealants, other caries prevention methods can be introduced to the patient.
Fluoride Alternatives
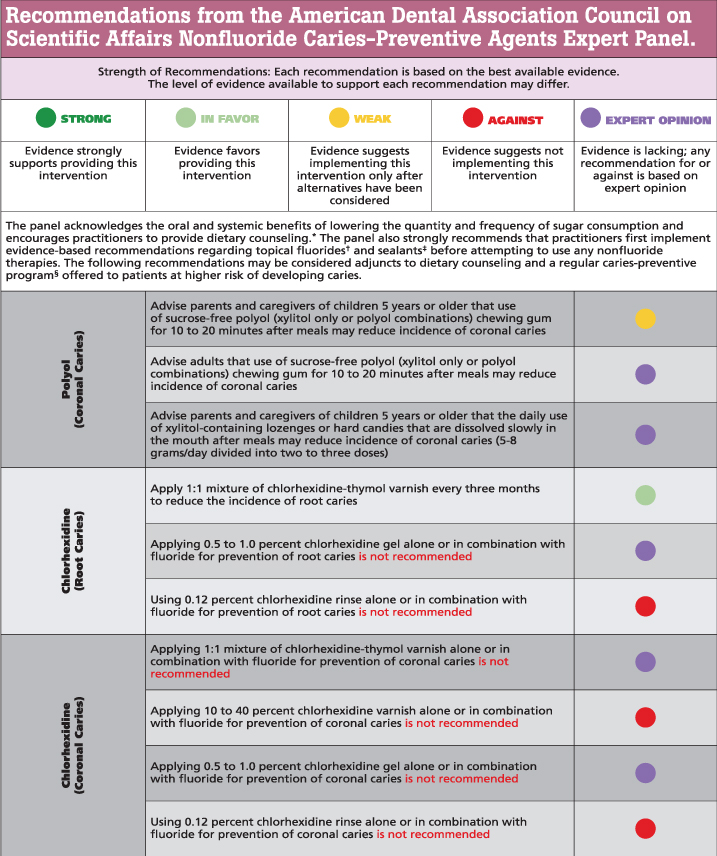
Possible alternatives to fluoride include non-fluoride caries preventive agents, sucrose-free polyol chewing gums, chlorhexidine rinse or gel, chlorhexidine-thymol varnish, and hydroxyapatite (calcium phosphate-based) dentifrices. According to research, there are varying levels of certainty or recommendation for using these non-fluoride agents 3.
Hydroxyapatite (HAP)
Hydroxyapatite (HAP) containing toothpaste or rinse is a newer product with some promise as a fluoride-free anti-caries agent.
Hydroxyapatite is a mineral composed of calcium and phosphate ions and is the principal organic component found in enamel. When these ions are lost from the tooth structure, demineralization of enamel occurs. Remineralization will happen when there are high calcium and phosphate ions in oral fluids.
The particle size of the calcium and phosphate ions in HAP-containing agents binds to the damaged enamel and fills the irregular tooth surface. HAP products are more beneficial in penetrating deeper into the tooth surface than fluorides, which are limited to surface remineralization.
HAP-containing agents have been tested in laboratory and human trials. The safety aspect of the products is high, and there is no risk of fluorosis. Although more research is needed to confirm its effectiveness in arresting caries, it suggests that it is equivalent to fluoride toothpaste. HAP-containing products may also reduce biofilm formation and serve as dentin desensitizers4.
Results from studies on the efficacy or benefit of non-fluoride agents may exist if they are used only as an adjunct to other proper caries control procedures in children and adults with a higher risk of developing new or recurrent carious lesions. Until further evidence supports the use of these products, clinicians must continue to recommend dental sealants, fluoride for at-home use in the form of toothpaste or rinses, and periodic professional fluoride application, as they remain the primary interventions effective in preventing caries3.
Conclusion
Fluoride has been proven safe to use, but some patients either need more information, or to be given an alternative such as hydroxyapatite and chlorhexidine rinse or gel. Talking with the patient and understanding their reasons for refusal of fluoride products can help in supporting patients to make the best decisions about it with the most up-to-date information.
maxill is proud to provide this information, along with everyday lowest prices on many great fluoride-based products such as prophy paste, fluoride varnish, fluoride rinses, and toothpaste.
Sources:
- Centers for Disease Control and Prevention. (n.d.). Statement on the Evidence Supporting the Safety and Effectiveness of Community Water Fluoridation. Community Water Fluoridation. https://www.cdc.gov/fluoridation/guidelines/cdc-statement-on-community-water-fluoridation.html
- Chi DL. Parent Refusal of Topical Fluoride for Their Children: Clinical Strategies and Future Research Priorities to Improve Evidence-Based Pediatric Dental Practice. Dent Clin North Am. 2017 Jul;61(3):607-617. doi: 10.1016/j.cden.2017.03.002. Epub 2017 May 4. PMID: 28577640; PMCID: PMC5783310.
- Michael P. Rethman, DDS, MS 1Eugenio D. Beltrán-Aguilar, DMD, MPH, MS, DrPH Et al.(2011). Non fluoride caries preventive agents. Executive summary of evidence-based clinical recommendations. The Journal of the American Dental Association, 142(9), 1065-1071. https://doi.org/10.14219/jada.archive.2011.0329
- O’Hagan-Wong, Kelsey & Enax, Joachim & Meyer, Frederic & Ganss, Bernhard. (2021). The use of hydroxyapatite toothpaste to prevent dental caries. Odontology. 110. 10.1007/s10266-021-00675-4.
Maryanne Ferree RDH, BS, PHDHP
Maryanne Ferree, BS, RDH, PHDHP, CDIPC from Pittsburgh, Pennsylvania, is a registered dental hygienist with over 39 years of experience. She has ventured into many facets of dental hygiene, including clinical care, public health, and education. She is currently a clinical faculty member in the Department of Periodontics and Preventive Dentistry at the University of Pittsburgh School of Dental Medicine focusing her clinical teaching on Periodontal Instrumentation. She has been excited to step into the role of KOL and blogger to share her enthusiasm for infection control in the dental setting, OSHA compliance training, and periodontal disease therapy.